Table of Contents
You already know the line.
“Mitochondria is the powerhouse of the cell.”
Every person who took biology in middle school has that burned into their brain. Teachers love saying it. Memes keep it alive.
And it tells you almost nothing useful.
Because if the mitochondria are the powerhouse, what does that actually mean for how you feel at 44? What does it mean for why your recovery takes longer than it used to? Why you hit a wall at 2pm every day even when you slept 8 hours?
Nobody connects those dots. So let me do it.
I have been in the peptide space for 10 years. I have run mitochondrial protocols on myself. But the moment that made this real for me was watching what happened to my mom.
She had not felt like herself in years. Very low energy and poor sleep, she just felt like she was running on empty. She thought that was just what getting older felt like
I put her on a full cycle of injectable NAD+ and MOTS-c.
Within a few weeks her energy started stabilizing. Recovery improved. She stopped hitting the wall mid-afternoon. By the end of the cycle she was a different person her words, not mine. Her sleep improved. She had energy she had not felt in years.
This is the breakdown I wish someone had given me when I started digging into this stuff.

Get Your Free Copy of The Ultimate Peptide Blueprint
Exact stacks, dosages & cutting-edge protocols to cut fat, build muscle, and keep results-no fluff.
No spam. Unsubscribe anytime.
What Mitochondria Actually Are
Your body is made of roughly 37 trillion cells. Most of those cells have mitochondria living inside them. Your heart cells might have 5,000 mitochondria per cell. Your muscle cells, thousands more. Your brain cells are loaded.
They earned the “powerhouse” label because they produce ATP. ATP is the energy currency your body runs on. Every time you lift a weight, think a thought, pump blood, or digest food, ATP is what makes it happen. Without ATP production, nothing works.
But calling mitochondria just an energy factory misses most of what they do.
Mitochondria also control apoptosis, which is programmed cell death. When a cell gets damaged beyond repair, mitochondria are the ones that signal it to shut down. That is a good thing. You want damaged cells eliminated before they cause problems.
They regulate calcium signaling, which affects muscle contraction and nerve transmission. They produce heat to maintain body temperature. They generate reactive oxygen species — which in small amounts are useful signaling molecules but in excess become the oxidative stress that damages tissue and accelerates aging.
And they communicate with your cell’s nucleus, influencing gene expression. Your mitochondria are sending signals that affect which genes get turned on and off.
This is not a simple power plant. It is closer to a command center.
What Happens to Mitochondria as You Age
This is where it gets personal because mitochondrial decline after 40 maps directly to symptoms most people just accept as “getting older.”
Around your mid-30s, mitochondrial function starts declining. By 40 it is measurable. By 50 it is significant. Research suggests that by 60, you have lost roughly half of your peak mitochondrial capacity.
Two things happen simultaneously.
First, you produce fewer mitochondria. The process that creates new mitochondria — called mitochondrial biogenesis — slows down. Your cells stop replacing old, worn-out mitochondria as efficiently. You end up with less total mitochondrial mass.
Second, the mitochondria you have become less efficient. The machinery inside them accumulates damage. They produce less ATP per cycle. They generate more oxidative stress as a byproduct. Signal quality degrades.
Fewer mitochondria. The ones that remain are worn down and underperforming. That combination is what makes 45 feel nothing like 25.

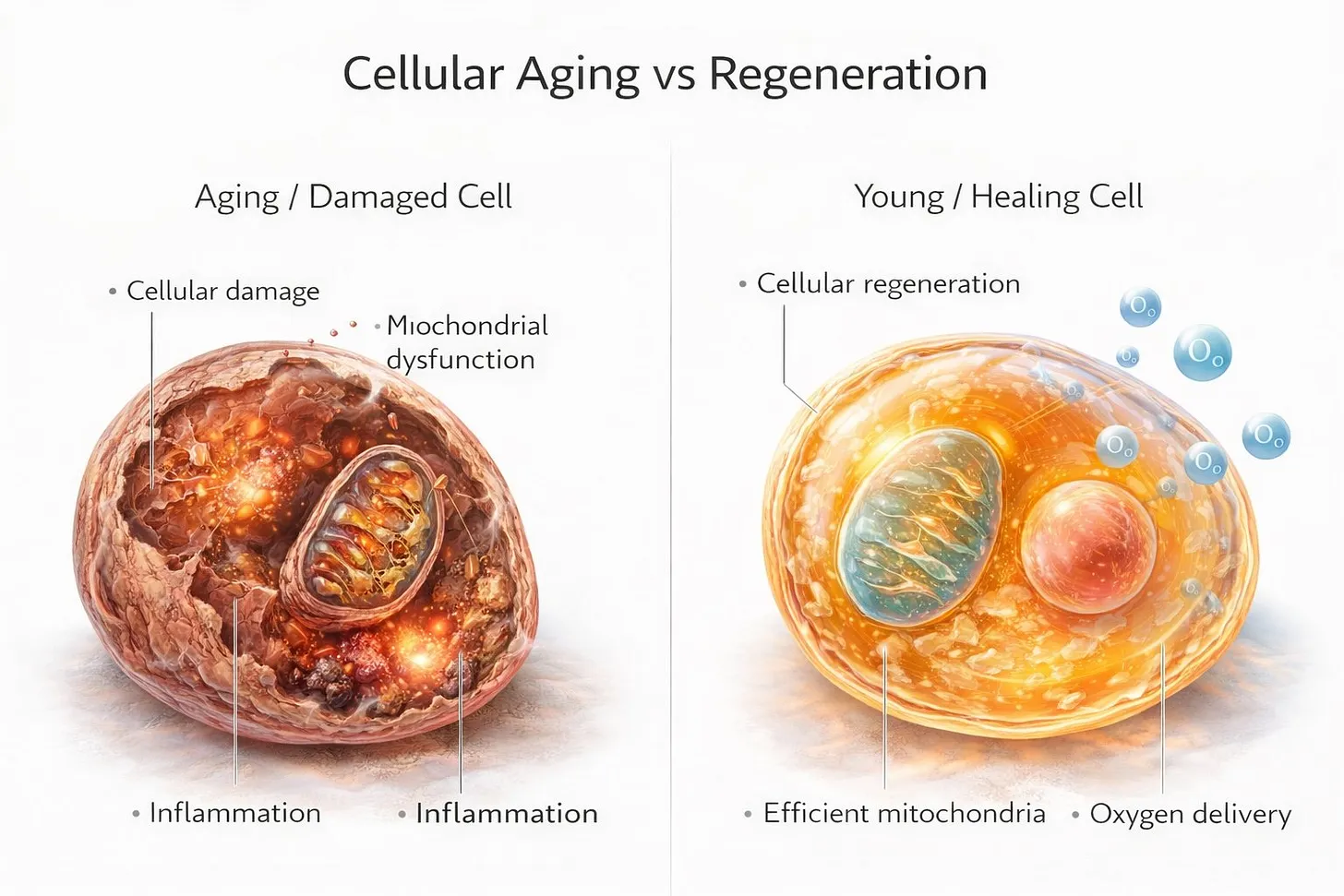
Now map that to real symptoms.
The afternoon energy crash that did not happen in your 20s is mitochondrial output declining. Recovery taking 3 days instead of 1 is mitochondria unable to keep up with cellular repair demands. Brain fog and slower thinking happen because your brain is your highest-energy organ and the first to feel the drop. Stubborn body fat, especially around the midsection, is mitochondrial dysfunction directly impairing fat oxidation and metabolic efficiency.
Feeling like you are running on 70% no matter how well you sleep or eat is not in your head. The cellular infrastructure is degrading.
This is why aging feels the way it feels. Not one dramatic moment. A slow erosion of cellular energy production happening across trillions of cells simultaneously.
The Fuel Problem: Why NAD+ Is the Foundation
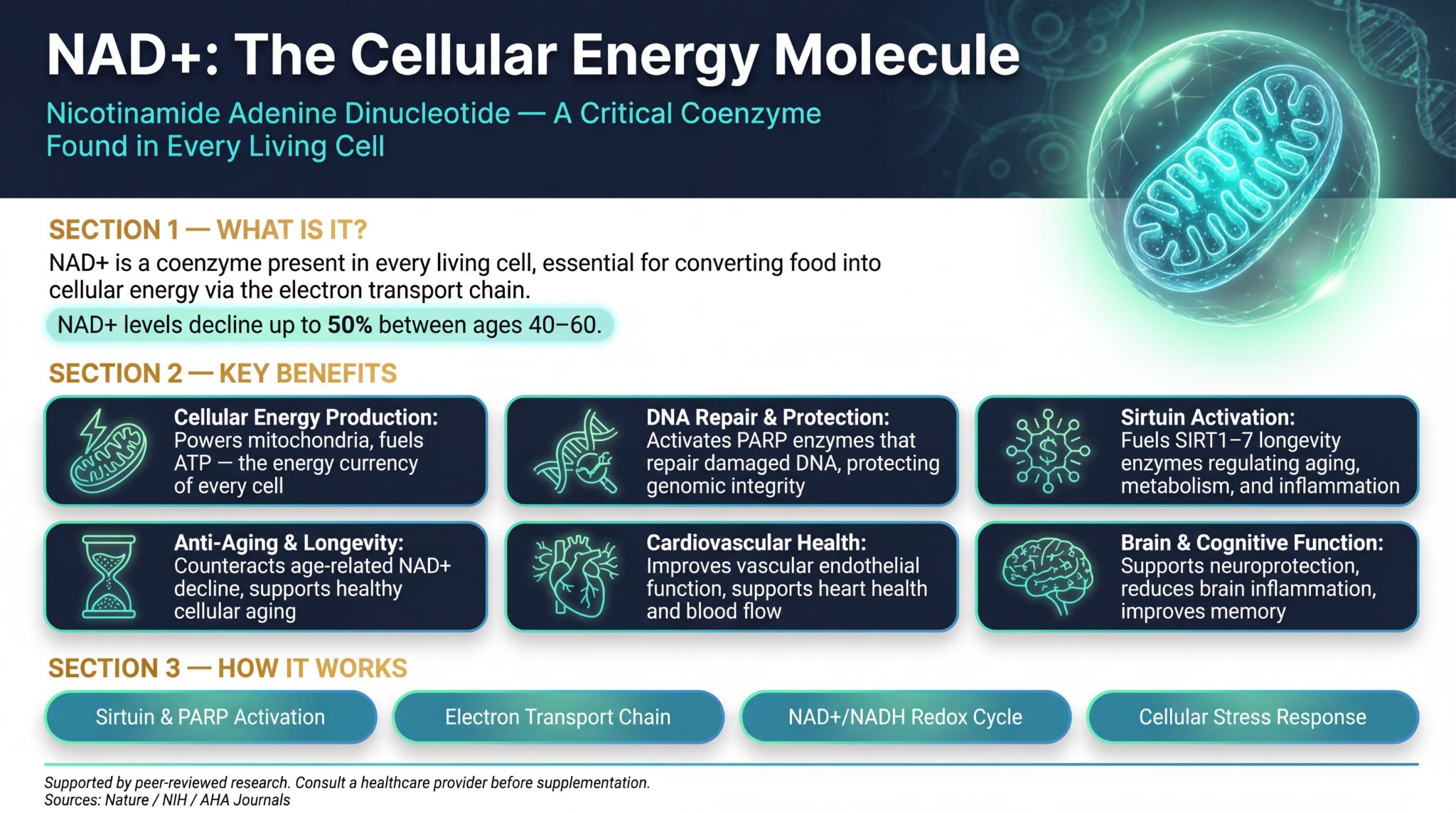
Your mitochondria run on a coenzyme called NAD+ — nicotinamide adenine dinucleotide. Think of NAD+ as the fuel your mitochondria need to actually function. Without it, the machinery stalls. Energy production drops. The repair pathways go offline.
NAD+ does three critical things inside your mitochondria.
It powers the electron transport chain — the actual process that converts food into ATP. No NAD+, no ATP.
It activates sirtuins. Sirtuins are proteins that regulate DNA repair, inflammation control, and cellular longevity. They require NAD+ to function. Without adequate NAD+, your sirtuins are sitting idle.
It supports PARP enzymes, which repair DNA damage. Every day your DNA takes hits. PARP repairs it. PARP runs on NAD+.
Your NAD+ levels drop roughly 50% between age 40 and 60. The same decade your mitochondrial function is already declining, you are also losing the primary fuel your mitochondria need to run. You cannot improve mitochondrial function without addressing NAD+ first. It is the foundation everything else builds on.
Why Injectable NAD+ Is Different From NMN and NR Supplements
This is one of the most common questions I get. Oral precursors like NMN and NR still have to convert inside the body before they become usable NAD+. You lose a significant amount in that conversion process. Injectable NAD+ bypasses the conversion steps entirely and delivers the compound directly.
The difference in how you feel it is meaningful. Oral supplementation is a slower, less direct path. Injectable SubQ gets you to therapeutic levels faster — which matters especially during the loading phase.
Understanding the NAD+ Loading Phase
Most people start a NAD+ protocol at a low maintenance dose and feel nothing after two weeks. Then they quit. This is the most common mistake.
If your levels have been depleted for years, starting at a maintenance dose is like dripping fuel into a tank that is running on empty. It works eventually but it takes a long time to cross the threshold where you actually feel something. The loading phase fills the tank fast.
You dose daily for 7-10 days to saturate your cells with NAD+ as quickly as possible. Once levels are restored you drop to a maintenance schedule — topping off a full tank rather than filling an empty one.
If you had strong sensitivity to IV NAD+ in the past, SubQ absorbs significantly slower. Start at 50mg daily for the first week and assess before pushing to 100mg.

Peptides can get expensive, but as an FYI - BioEdge is doing 15% off this month (code mars15 at bioedgepeptides.com), one of the few suppliers that consistently delivers what their lab reports claim.
| NAD+ Phase | Protocol Details |
|---|---|
| Loading Phase | 100-200mg SubQ daily for 7-10 days |
| Loading (sensitive individuals) | Start at 50mg daily, assess at day 7 |
| Maintenance | 100-200mg SubQ, 2-3 times per week |
| How to determine 2 vs 3 days | Start at 2x/week. If energy dips mid-week before next injection, move to 3x |
| Timing | Morning only — NAD+ is energizing and can interfere with sleep |
| Max SubQ dose | 200mg — above this increases nausea and flushing risk |
| Cycling | Continuous — no cycling needed. Adjust frequency based on how you feel |
The Building Problem: What MOTS-c Actually Does
NAD+ restores and fuels your existing mitochondria. That is essential. But it does not solve the other half of the problem — the fact that you have fewer mitochondria than you used to.
That is where MOTS-c comes in.
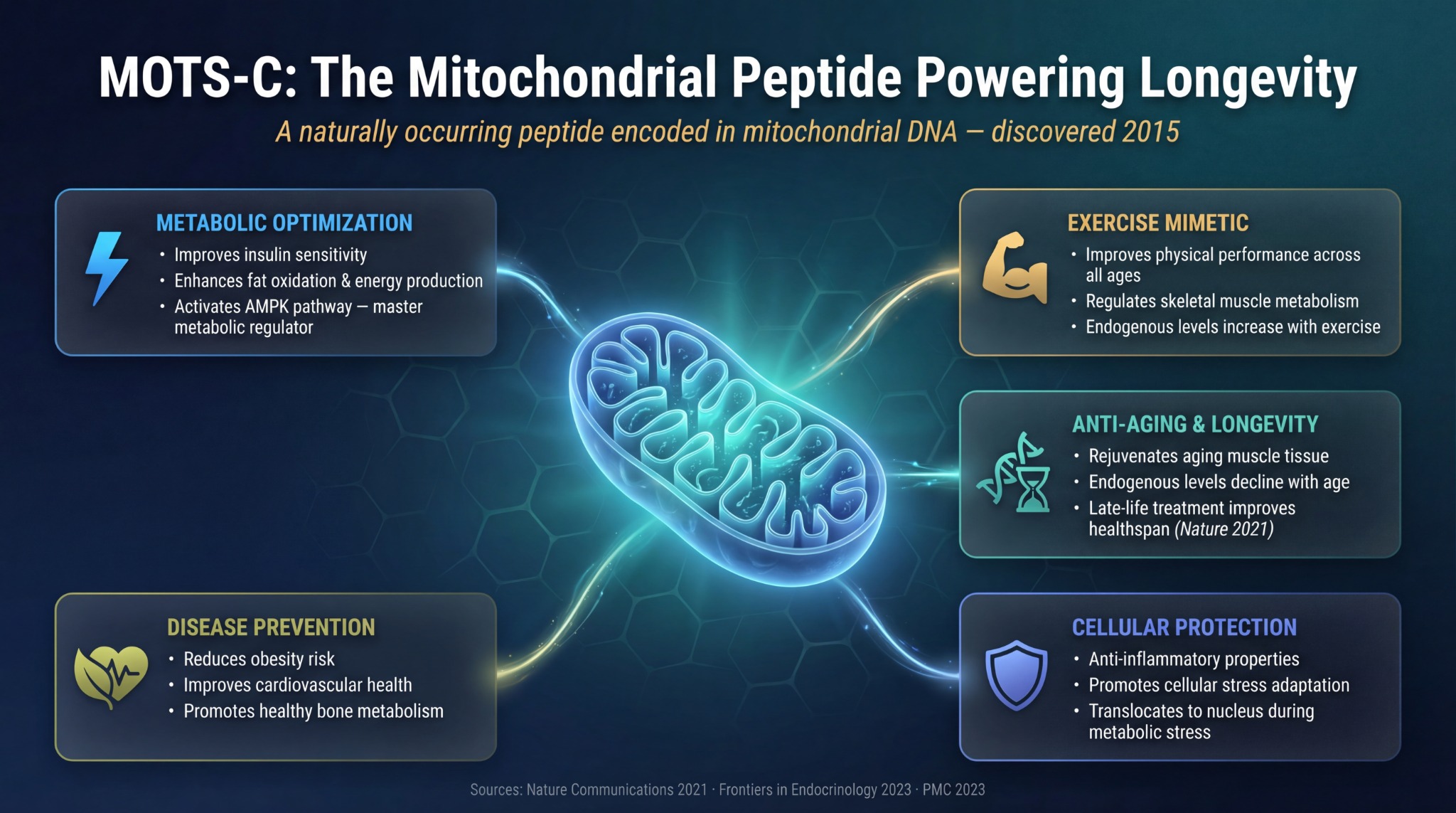
MOTS-c is a mitochondrial-derived peptide, meaning it is literally encoded by your mitochondrial DNA. It was first identified in 2015. Research from MOTS-c levels in 70-81 year olds shows they drop nearly 21% compared to 18-30 year olds — so the decline is measurable and significant.
MOTS-c activates AMPK — AMP-activated protein kinase — which is a master metabolic regulator. When AMPK gets activated, a cascade follows:
- Mitochondrial biogenesis is triggered — your body signals the creation of new mitochondria. You are not just working with what you have. You are building more.
- Insulin sensitivity improves — your cells take up glucose more efficiently, feeding directly into better energy production.
- Fat oxidation increases — your body gets better at burning fat as fuel.
- Inflammation decreases at the cellular level — MOTS-c has been shown to downregulate pro-inflammatory cytokines including IL-6, IL-1β, and TNF-α.
- Stress resilience improves — under metabolic stress, MOTS-c translocates to the nucleus and regulates gene expression to promote cellular balance.
Some researchers describe MOTS-c as mimicking the cellular response to intense exercise — specifically the mitochondrial growth signal you get from hard training. The research out of Nature Communications 2021 showed late-life MOTS-c treatment improved healthspan in animal models.
| MOTS-c Parameter | Details |
|---|---|
| Dose | 5mg |
| Frequency | 3x weekly (Monday, Wednesday, Friday) |
| Route | Subcutaneous injection |
| Timing | Morning — same day as NAD+ injection |
| Cycle Length | 10 weeks on, 4-6 weeks off |
| Stack compatibility | Compatible with Reta, CJC/IPA, BPC-157 — no conflicts |
MOTS-c is a research peptide. Human studies are still developing. What we understand comes primarily from preclinical research and early human data. This is for research purposes only.
Why NAD+ and MOTS-c Work Better Together
NAD+ and MOTS-c address mitochondrial decline from opposite directions — and that is exactly why the combination is more effective than either alone.
NAD+ works on what you have. It restores the fuel supply, activates the repair proteins, and brings existing mitochondria back toward peak function. Think of it as getting the current engines running at full power again.
MOTS-c works on what you are building. It signals your body to create new mitochondria and improves how efficiently those mitochondria operate. More engines, better performance.
Research has established that NAD+ and MOTS-c share overlapping metabolic pathways. MOTS-c has been shown to play a role in increasing NAD+ levels — meaning they reinforce each other’s effects. One study specifically noted that MOTS-c treatment reduced an enzyme called Cd38 that consumes NAD+, which effectively allows NAD+ levels to stay higher for longer.
Together they cover both sides of the mitochondrial decline problem. More mitochondria, all running with the fuel and repair systems they need to actually perform.
How to Run Both Together
| Day | Protocol |
|---|---|
| Monday | NAD+ (loading or maintenance dose) + MOTS-c 5mg — both in the morning |
| Tuesday | NAD+ only (loading phase) — or rest day (maintenance phase) |
| Wednesday | NAD+ + MOTS-c 5mg — both in the morning |
| Thursday | NAD+ only (loading phase) — or rest day (maintenance phase) |
| Friday | NAD+ + MOTS-c 5mg — both in the morning |
| Weekend | NAD+ only (loading phase) — or rest days (maintenance phase) |
Always inject both in the morning. NAD+ is energizing at the cellular level — injecting in the afternoon or evening can interfere with sleep. Rotate injection sites to avoid tissue irritation.
What to Expect Week by Week
Mitochondrial peptides are not like GLP-1s or healing peptides where you feel something in the first few days. They work cumulatively. Here is what the realistic timeline looks like:
| Timeframe | What to Expect |
|---|---|
| Days 1-7 (loading) | Some people notice increased alertness or mental clarity. Others feel nothing yet. Both are normal. |
| Weeks 2-3 | Subtle improvements in energy consistency. Possibly better sleep quality. Afternoon crashes start to improve. |
| Weeks 4-5 | Energy more stable throughout the day. Recovery windows noticeably shorter. Mental stamina improving. |
| Weeks 6-8 | Clear difference in training capacity. Afternoon crashes mostly gone. Overall sense of vitality increasing. |
| Weeks 8-10 | Full cumulative benefits. Recovery significantly faster. Body composition improvements visible with proper diet and training. |
The key is consistency. These are not peptides you run for two weeks and expect dramatic results from. The people who quit at week 3 never get to see what the protocol actually does.
Frequently Asked Questions
The Takeaway on Mitochondrial Decline
Mitochondria are not just energy factories. They regulate cell death, inflammation, metabolism, gene expression, and aging at the cellular level.
By the time most people hit their mid-40s both problems are already in motion — they have fewer mitochondria, and the ones left are underperforming.
The fuel problem is real. NAD+ depletion is measurable and begins earlier than most people think.
The building problem is real. Mitochondrial biogenesis slows, MOTS-c levels fall, and new mitochondria stop replacing old ones fast enough.
Both problems have research-backed approaches. Neither is a cure. Both are worth understanding if you take your cellular health seriously.
I will keep breaking this down as the research develops.
Stay sharp,
Joe Mars | The Peptide Report
P.S. — Join Our Peptides and Biohacking Hub on Skool — this is where I answer protocol questions, share what I am personally running, and go deeper on everything covered in this article.
All content on The Peptide Report is for educational and informational purposes only. Nothing here constitutes medical advice. All peptides discussed are research compounds. Consult a qualified healthcare provider before beginning any peptide protocol.
Peptides can get expensive, but as an FYI - BioEdge is doing 15% off this month (code mars15 at bioedgepeptides.com), one of the few suppliers that consistently delivers what their lab reports claim.